
Bells Palsy
Understanding Bell’s Palsy
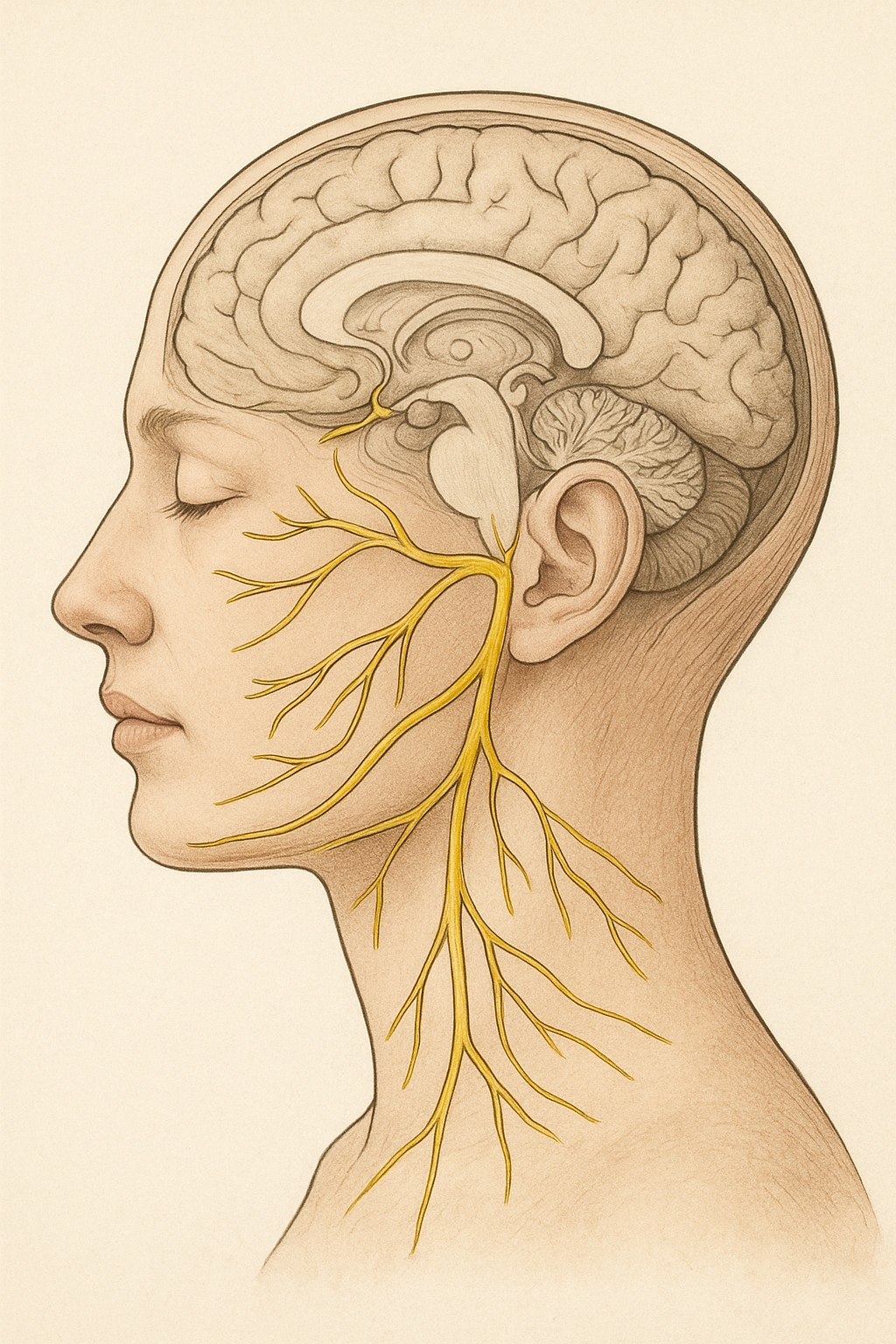
What is Bell’s Palsy?
Bell’s Palsy accounts for around 60% of all facial nerve cases. There is around a 1 in 60 chance of developing it in one’s lifetime with increased chances during pregnancy or with a history of T2 diabetes. It causes sudden weakness or paralysis of the muscles on one side of your face. This happens when the facial nerve (cranial nerve 7), which controls those muscles, becomes inflamed or compressed while the nerve is still inside a very long bony tunnel. It may cause your face to droop, and you may have trouble smiling, closing your eye, or eating and drinking. To get really dorky - it’s a transient (often not permanent) idiopathic (diagnosis of exclusion) mononeuropathy (damage to 1 nerve) of the facial nerve. The recurrence rate of Bell’s Palsy is between 3-15%.
Bell’s Palsy is not caused by a stroke, and it usually affects just one side of the face. You will usually be checked for a stroke when you present to your GP or ED.
It is important to know that complete flaccid/floppy paralysis is normal, not reflective of degree of damage and is usually at its worst at 3 days in irrespective of medication. That is just the natural progression of the condition.
What Causes Bell’s Palsy?
The exact cause isn’t always clear, but it’s often linked to:
- Viral infections (in the family of chicken pox or cold sore virus’)
- Changes to the blood supply around the facial nerve
- Inflammation of the facial nerve
- Some people who have this multiple times have different anatomy that makes the nerve naturally a bit touchy to inflammation
There was nothing that you did wrong or could have done to prevent it happening.
What Is the Prognosis?
The outlook for Bell’s Palsy is generally very good:
- Most people (70–90%) recover fully within 3 to 6 months.
- Some may have lingering symptoms like facial weakness or tightness.
- A small number may have ongoing symptoms or develop synkinesis.
What is normal and what to expect:
The markers we look for in a Bells palsy recovery are 3 days, 3 weeks and 3 months.
Your condition will be at it’s worse at day 3 (irrespective of medication), it is NORMAL to have a complete flaccid (floppy) paralysis. This is not a reflection of severity.
If you have a flicker of movement in the first 3 weeks, we can prognosticate that you should be on a normal bell curve trajectory for BP. We would expect you to be almost completely better at 3 around months. Nerves are temperamental and it can be hard to predict at times.
Medical Management
You need to see a doctor! And depending on your recovery we may send you to a facial nerve specialist for extra help.
Treatment often includes:
Steroids (such as prednisone): Help reduce nerve inflammation and improve recovery.
Antiviral medications (in some cases): If a virus is suspected.
Pain relievers: To ease discomfort or ear pain.
Early treatment (within 72 hours) gives the best chance for full recovery.
If you are suspicious of hearing LOSS a hearing test referral can be done to establish if help is needed
Eye Care Is Very Important
When you have Bell’s Palsy, your eye on the affected side may not close completely. This puts it at risk of dryness, irritation, or injury.
To protect it:
Use Eye drops during the day to keep your eye moist. These should be preservative free.
Apply lubricating ointment at night.
You can use an eye patch, glad seal and press or tape your eyelid shut at night if it doesn’t close. Your physio will show you how to do this
Wear sunglasses during the day to protect from wind and the sun. The bigger the better.
Pharmacists can help you with drops, optometrist and ophthalmologists can check on your eye health and advise on specific drops and care options.
Normal Symptoms:
Pain around or behind the ear: Often starts before onset of the paralysis and is usually gone by 4-6 weeks
Complete facial palsy: it is NORMAL to be completely paralysed, some people may be incomplete. Slow progressive paralysis or incomplete paralysis warrants more investigation.
The paralysis is FAST, usually happening over a day or a few hours. Slow progressive weakness over weeks or months or weakness that comes and goes IS NOT BP.
Change in taste: a metallic taste or loss of taste on the affected side can start before the paralysis and usually subsides in the first 4-6 weeks
Hyperacusis (increased sensitivity to sound): loud noises wont feel great! Again this usually settles in the first 4-6 weeks. Hearing loss and loss of balance are NOT features of BP.
Fatigue in yourself and your face: This is a decent injury. You will feel more tired than usually in the first month or 2 and while you face is recovering. Be nice to yourself!
The Role of Physiotherapy
Physiotherapy can be very helpful in your recovery. A specially trained physiotherapist can:
- Teach gentle facial exercises to help facilitate quality of movement return
- Guide you in massage techniques to reduce tightness
- Help reduce or manage synkinesis in conjunction with facial nerve specialists
- Ensure we have you recovering in the correct time frames and facilitate referrals at appropriate times.
It’s important to start physiotherapy once the facial nerve has started to recover. Doing exercises too early or incorrectly can sometimes cause problems. We are happy to see you in the flaccid/floppy/paralysed phase to check in and make sure you feel confident with what to do and what to expect.
Things to Avoid:
- Overzealous exercise when your face doesn’t move
- Taking pictures daily – try for once every week to 2 weeks if this is something you would like to do
- General electrical stimulation, or electroacupuncture
.